
Surgical Treatment
Surgery is an important consideration in the effective treatment of breast cancer. With the continuing developments of breast cancer treatment, surgery today is less disfiguring. Options for local treatment include total mastectomy or breast-conserving surgery, axillary sentinel lymph node biopsy or removal. Women who have a mastectomy may also decide to have breast reconstruction, either at the same time or at a later stage.
Total mastectomy
In this procedure the surgeon removes the entire breast, including the nipple, and the skin above the tumour (Figure 1). When axillary lymph node (level 2 axillary dissection) is removed in continuity with a total mastectomy, it is called modified radical mastectomy. As modified radical mastectomy preserves chest wall muscle and part of the lymph nodes (level 3 ) in the axilla, women are therefore left with a stronger arm and less disfigurement.
Women undergoing a mastectomy have the option of reconstruction either at the same time, or at a later stage. Implant or tissue from other body parts can be used for reconstruction (Figure 2). For suitable cases, skin sparing mastectomy or nipple areola-sparing mastectomy, which leaves the shell of skin or nipple areola complex in place, allows a more natural looking breast with reconstruction.
Only part of the affected breast is removed, i.e. lumpectomy or quadrantectomy (Figure 3). Axillary surgery is usually performed together, and radiotherapy is given after surgery to eradicate any residual subclinical tumour in the affected breast.
Lumpectomy removes the main tumour and a surrounding margin of normal tissue. Quadrantectomy removes more breast tissue than a lumpectomy as one-quarter of the breast is removed.
Oncoplastic Surgery
With the advance of oncoplastic surgery, local plastic surgery techniques are integrated into reshaping of the breast after breast conserving surgery. These include the raising of breast glandular flaps by undermining the overlying skin envelope and underlying pectoral muscles. This development has allowed the extended use of breast conserving surgery in tumours located in unfavourable areas, such as medial or inferior tumours, and tumour size that might previously be thought not suitable for breast conserving surgery.
Goals of Reconstruction
The main aim is to restore breast symmetry, contour and volume. Ideally, the contralateral breast should be left intact for better cancer monitoring. The method of reconstruction is determined by the overall health of patient, size and shape of opposite breast, volume of tissue available from the abdomen or upper back chest wall, amount of residual skin after mastectomy, patient's preference (autologous tissue versus implants), and the stage of breast cancer. The best alternative is determined before surgery after consulting the oncologist, reconstructive surgeon, and patient in a three-way dialogue.
Choosing between Mastectomy or Breast Conserving Surgery
When deciding between mastectomy or breast conserving surgery, it is important the patient is consulted and evaluated carefully by a breast surgeon. Individual situation and special needs should be discussed so that the best treatment option is tailored to the woman to achieve cosmetically satisfactory breast shape without jeopardizing survival or local recurrence.
In some women, breast conserving surgery is usually not recommended if they have any one of the below conditions:
- previous radiotherapy to the affected breast
- two or more areas of cancer in the same breast that are far apart
- persistent positive margins after reasonable attempts of re-excision(s)
- serious connective tissue disease(s), and therefore tolerate radiotherapy poorly
- Pregnancy and therefore cannot have radiotherapy
- large tumour relative to breast size, and the tumour doesn't shrink well with neoadjuvant chemotherapy
There are some misconceptions about breast conserving surgery. Many women believe that if mastectomy is chosen, further radiotherapy or chemotherapy will not be necessary. In fact, a certain percentage of women undergoing mastectomy still require radiotherapy. As for the need for chemotherapy, this will depend on lots of other factors rather than the extent of the surgery. Chemotherapy, as well as the extent of surgery for the lymph nodes is the same whether breast conserving surgery or a mastectomy is performed.
Sentinel Lymph Nodes Biopsy
The sentinel lymph node is the first lymph node to receive lymph fluid from the area of the breast. When cancer cells begin to move along the lymphatic channels from a primary tumour in the breast, they will first reside in the sentinel lymph node. Subsequently, tumour cells will spread from the sentinel lymph node to other lymph nodes in the axilla. In 95% of cases, if there are no tumour cells in the sentinel lymph node, all the other lymph nodes will be clear. Sentinel lymph node biopsy is the removal of the sentinel lymph nodes. The lymph nodes are then examined for tumour cells.
Not every breast cancer patient is suitable to undergo sentinel lymph node biopsy. The most suitable patient is one who has a small and solitary primary tumour, and for whom physical examination and/or other imaging modalities do not show any suspicious lymph nodes in the drainage area of the breast.
Surgical Treatment Can Boost Self-confidence
With the advance in multi-modality treatment, breast cancer surgery is aiming to achieve best possible results for women while restoring as much of their normal function and appearance as possible. Retaining the breast shape through breast conserving surgery or restoring body appearance by reconstruction is proven to be safe and is important for the psycho-social wellbeing of women with breast cancer.
Special thanks to:
Dr. Sharon Chan Wing-Wai
Clinical Director, Kowloon East Cluster Breast Centre, United Christian Hospital
Dr. Miranda Chan
Chief of Service, Department of Surgery, Kwong Wah Hospital
Dr. Kenneth Hui
Specialist in Plastic Surgery
Figure 1: Total Mastectomy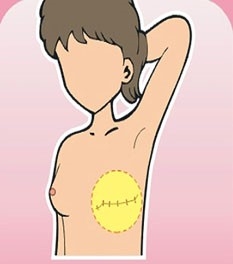
Figure 2: Breast Reconstruction
| Implant | Latissimus Dorsi Flap (LD flap) | Pedicled Transverse Rectus Abdominis Myocutaneous Flap (TRAM flap) |
 |
 |
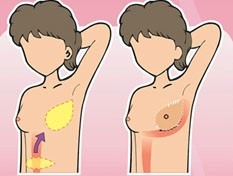 |
Figure 3: Breast Conserving Surgery

10/2014